


The perverse incentives of euthanasia
Suggesting that people die is not a good way of saving taxpayer money.


“The mayor’s out killing kids/ To keep taxes down” — The Weakerthans
Today’s post is about a sensitive and difficult topic: euthanasia, also known as “assisted dying”.
I do think euthanasia is OK in principle. I believe that as long as they’re in their right mind, people have the right to die instead of continuing to live in horrible pain. The idea does not disgust me, or trigger a deep-seated moral taboo. If you disagree with that — if you think that all human life is sacred and should be preserved and protected at any cost, or even if you just feel like there’s something wrong with euthanasia that you can’t quite express — then fine. I respect that viewpoint. That’s not the debate I want to have today.
What I do want to talk about today are some very important perverse incentives that any euthanasia policy needs to work strenuously to avoid. And watching the progress of Medical Assistance In Dying (MAID) in Canada and the discussion about it in the UK, I’m doubtful that even the most responsible, morally beneficent policymakers and professionals can entirely avoid those incentives on their own.
The basic problem is that promoting wider use of euthanasia could save money for taxpayers and the health care system. A 2017 paper by Trachtenberg and Manns in the Canadian Medical Journal finds:
Using published data from the Netherlands and Belgium, where medically assisted death is legal, we estimated that…Medical assistance in dying could reduce annual health care spending across Canada by between $34.7 million and $138.8 million, exceeding the $1.5–$14.8 million in direct costs associated with its implementation.
Now, even the upper estimates here are not a lot of money. Canada spends $331 billion a year on health care, so saving $137 million would be about 0.04% of that. Other papers have found similar numbers.
But just because a financial incentive seems small doesn’t mean it’s not important. First of all, those savings might be highly concentrated; to some specific hospitals or other providers choosing whether or not to offer more patients euthanasia, the incentive might not be small.
Second of all, and more important, existing cost savings are not the same as potential cost savings. Trachtenberg and Manns note that most euthanasia recipients are very close to the end of their life; cost savings are small because most of the patients were about to die anyway. But if euthanasia is allowed to expand to lots of people who aren’t about to die, the cost savings could grow by a lot.
After all, health spending is fairly highly concentrated among a small segment of the population:
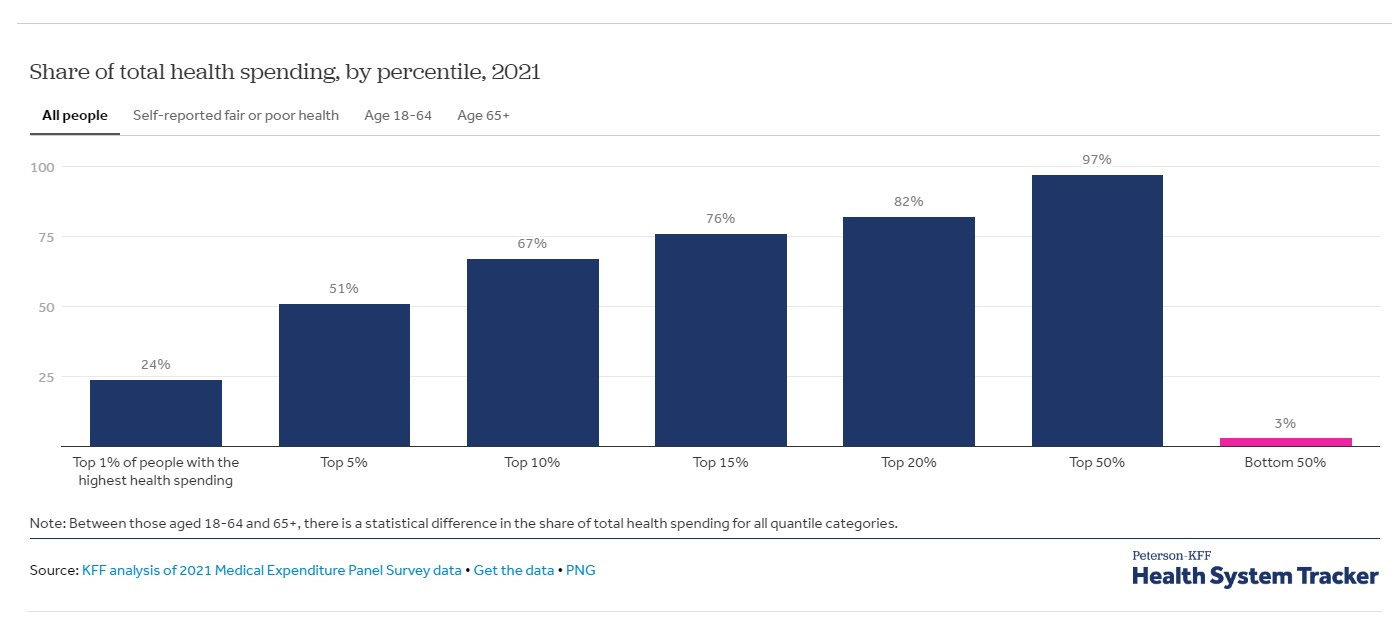
If more of those top 1% of spenders used MAID, those millions of dollars in health costs savings could turn into billions. It’s those potential future savings, not current savings, that create the incentive to expand the euthanasia system to an abusive degree.
And there’s no guarantee that euthanasia usage will remain within past limits. Canada’s MAID program is growing — assisted suicides represented 4.1% of all Canadian deaths in 2022, which is already a little bit over the maximum estimate of Trachtenberg and Manns (2017). That represents an astounding 31.2% growth rate compared to 2021. Even in the Netherlands and Belgium, euthanasia has been growing rapidly, and is now well above the rate that Trachtenberg and Manns used for reference in their paper seven years ago.
Finally, what really matters in terms of the financial incentive to overuse euthanasia is the perceived incentive. In a recent op-ed in the British newspaper The Times, entitled “We can’t afford a taboo on assisted dying”, Matthew Parris writes the following:
What today is criminal could tomorrow become (as its proponents tend to insist) a sad but permitted option in a relatively small number of special and agonising circumstances; but within a decade or more be seen as a normal road for many to take, and considered socially responsible — and even, finally, urged upon people. Such (say objectors) is the wedge of which the Scottish [euthanasia legalization] proposal is just the thin end.
Yes, but what’s wrong with the thick end? It will be a healthy development. In this century the future holds an almost cosmic struggle between, on the one hand, the old world with our ageing populations and inflexible economies, and, on the other, the raw and unbridled energies of an emerging, younger, nimbler and very different world, led by countries like China: all relatively new to prosperity and unencumbered by our western populations’ sense of entitlement…
It may sound brutal, but I don’t apologise for the reductivist tone in which this column treats human beings as units — in deficit or surplus to the collective…“Your time is up” will never be an order, but — yes, the objectors are right — may one day be the kind of unspoken hint that everybody understands. And that’s a good thing.
This language, frankly, disgusted me and chilled me to the bone — not because I find euthanasia itself disgusting, but because the idea of nudging old people toward death for the purpose of strengthening a nation relative to its rivals is antithetical to every value I hold dear. This is the kind of savage, brutal collectivism that liberal societies exist to protect people from in the first place — euthanasia as eugenics.
But the real point here is that if one British op-ed writer is saying it, you can bet that others are thinking it. Although everyone who supports euthanasia will obviously say they support it purely for the well-being of the recipients, some will secretly be thinking about their own interests. Parris’ op-ed is the most repugnant argument I’ve read in favor of saving money by expanding euthanasia, but it’s not the only one.
So there is definitely a perceived financial incentive for the expansion of euthanasia. The next question is what it would mean to expand the practice so much that it becomes abusive.
First, there’s the possibility that people could simply be denied life-saving treatments if health providers consider MAID a cheaper, acceptable alternative. The moral justification for MAID is based on the idea that people should get to choose when to die with dignity. But some people don’t want to choose death. If a health care system makes that decision for them, refusing to pay for non-MAID care, it has violated the principle that death should be a choice.
For example, here’s a story from last year about a Canadian woman who was given a poor abdominal cancer prognosis and urged to die with MAID instead of getting surgery and chemotherapy. She refused, and went to the U.S. for treatment. Canadian health insurance refused to pay for the treatment:
[Allison] Ducluzeau said her family doctor told her that with this type of cancer, they usually do a [surgery] which involves delivering high doses of chemotherapy into the abdomen to kill the cancer cells. But when she saw the consulting surgeon at the BC Cancer Agency in January, she said she was told she was not a candidate for surgery…
Ducluzeau said the surgeon told her…“[Y]ou have a life span of what looks like to be two months to two years. And I suggest you talk to your family…talk to them about your wishes…you know, whether you want to have medically assisted dying or not.”…
It was then that Ducluzeau promised herself to do everything she could to find another treatment and a better outcome…Ducluzeau decided to get treatment with [Dr. Armando] Sardi in Baltimore…Ducluzeau said she spent more than $200,000 for the surgery, chemotherapy, scans, travel and accommodation…Ducluzeau said she is doing well now and thanks the team at Mercy Medical Center for their care…
HIPEC is considered the standard for Ducluzeau’s cancer when possible but a letter from the BC Cancer Agency does not agree with this assessment.
Ducluzeau is trying to apply to have her medical bills funded by BC Cancer…However, the letter states “the services you chose to receive in the U.S. would not have been the recommended treatment for your cancer diagnosis.”
It’s not clear whether Ducluzeau will live a long life as the result of her treatment, but it’s possible. Now consider if she had been poor. She wouldn’t have had the $200,000 to fly to a different country and get treatment. She would have had little choice but to accept euthanasia instead.
It’s not 100% certain that financial incentives were involved in the Canadian health care system’s decision to deny Allison Ducluzeau the treatment that might have saved her life, and to instead urge her to kill herself. But given the system’s refusal to pay for her treatment, it certainly seems likely that cost was a consideration here.
It’s cases like Ducluzeau’s that have caused the proliferation of memes like this one:
But this isn’t all. There are other cases in which financial incentives could lead doctors to suggest euthanasia to people who are not mentally competent to make the decision of whether or not to die.
I have personally struggled with depression for a significant portion of my life, and I’m happy to say that I have never once contemplated suicide or felt like I wanted to die. But if I had gone to a medical provider while I was depressed, and they had suggested it as an option, I don’t have 100% confidence that I would have refused.
When a doctor offers you a treatment, it’s never just informing you of your options. It’s always a recommendation. It’s always a statement that this is one of the treatments that experts, authorities, medical science, etc. considers among the appropriate set of measures to address your condition.
And having been a depressed person, I can tell you with confidence that depressed people are not fully capable of pushing back against a doctor’s suggestions. Depression — at least, the kind that I suffered — entails a lack of volition, willpower, and motivation. When I was depressed, I would go along with other people’s suggestions, simply because I didn’t have any motivation to do anything other than go along. Fortunately, nobody suggested self-harm to me. But if a doctor had suggested that I’d be better off dead, I can’t tell you with 100% certainty that I would have had the wherewithal to gainsay them.
Depressed people also have great difficulty thinking rationally about what would actually improve their lives. When I was depressed, the entire notion of “feeling better” became abstract and a bit meaningless; I simply couldn’t imagine feeling anything different than I was feeling at the time. I’m a fairly happy person now, but while I was depressed, there’s no way I could have anticipated eventually becoming a happy person, or even conceived of it. So if a doctor had offered me euthanasia while I was depressed, I don’t think I would have been able to envision the future benefits of choosing to refuse that offer.
In other words, some people simply aren’t in their right mind, and thus aren’t equipped to make the choice of whether to die. Lots of people intuitively realize this, which is why Canada has temporarily delayed its plan to authorize MAID for the mentally ill. Still, there are isolated incidents in Canada that suggest that the practice is leaking into the system already. For example, here’s a story from 2022:
Alan Nichols had a history of depression and other medical issues, but none were life-threatening. When the 61-year-old Canadian was hospitalized in June 2019 over fears he might be suicidal, he asked his brother to “bust him out” as soon as possible.
Within a month, Nichols submitted a request to be euthanized and he was killed, despite concerns raised by his family and a nurse practitioner.
His application for euthanasia listed only one health condition as the reason for his request to die: hearing loss.
Nichols’ family reported the case to police and health authorities, arguing that he lacked the capacity to understand the process…They say…that hospital staffers improperly helped him request euthanasia…“Alan was basically put to death,” his brother Gary Nichols said…
Here’s a case of a Dutch woman was euthanized for depression after claiming that her doctors told her “It’s never gonna get any better.” And here’s a case from just last month in which a 27-year-old autistic Canadian woman with no known physical symptoms was granted euthanasia.
I have no idea whether saving taxpayer money was part of the motivation for these decisions. But the financial incentive to push the mentally ill toward death is certainly there, and it is enormous. Depression alone, for example, costs hundreds of billions of dollars to treat ever year in the U.S. Saving even a small fraction of that by making euthanasia a standard “treatment” for depression could result in a gigantic windfall for the taxpayer, as well as culling people that folks like Matthew Parris consider socially useless.
Yet this would, in my opinion, be a monstrous crime.
The perverse financial incentives of euthanasia seem both insidious and pervasive; when someone’s illness makes them a net financial burden on society, it is simply cheaper to kill them than to help them. This fact will always be present, consciously, or unconsciously, in the minds of doctors, insurers, and anyone else who has the power to push financially or mentally vulnerable toward suicide.
We can hope that the moral uprightness of doctors and bureaucrats will be enough to overcome that incentive every time, and that health care providers and insurers will never make their decisions based on anything except the patient’s well-being. But there are human beings we’re talking about, and depending on the moral fiber of human beings to win out over financial incentives every single time is a bad bet.
Note, by the way, that this is not a “slippery slope” argument. A “slippery slope” argument is the claim that any increase in permissiveness will automatically lead to further increases in permissiveness. Obviously, some kind of justification, whether theoretical or empirical, is needed in order to make such a prediction. But in the case of euthanasia, we have a good justification — the financial incentive for the expansion of assisted dying is plain to see, and people are talking about it in the newspapers. And there are clearly some very questionable cases of euthanasia going on in Canada.
In my view, we shouldn’t wait for questionable euthanasia cases to become the norm before we begin to be concerned. We can already see the problems coming, and so we should act on them before lots of vulnerable people die unnecessarily.
The first thing to do, I think, is to modify euthanasia policies to avoid the types of abuse cases that the articles above suggest. This would include, at the very least:
Keeping the rule that mental illness alone is not grounds for euthanasia
Stipulating that insurance coverage for treatments can never be denied on the grounds that MAID was offered as an alternative
Mandating training for doctors and insurers in which they have to agree that MAID should never be done in order to save money
Implementing oversight for MAID cases in which mental disability may be involved, in which multiple mental health experts have to sign off
Dismissal of (and, potentially, prosecution of) medical workers who pressure patients to be euthanized for financial reasons
An even stronger safeguard would be to stipulate that doctors and other care providers are never allowed to suggest MAID to patients who don’t ask about it on their own. This would ensure that no one ever feels that death is being recommended to them over other options, or that they’re being pressured into killing themselves.
Defenders of euthanasia systems like Canada’s may be tempted to circle the wagons, labeling anyone who raises these concerns as a right-winger or an opponent of public health care. That would be a mistake. If MAID is subject to such widespread abuses that it discredits the very idea of “death with dignity”, it will be to absolutely no one’s benefit. The perverse incentive here is very real, and you can’t just ignore it and hope it goes away.
Update: Here’s another excerpt from the AP article that I quoted above, which suggests that in at least a few cases, euthanasia is clearly being urged on patients, with an explicitly financial justification:
Roger Foley, who has a degenerative brain disorder and is hospitalized in London, Ontario, was so alarmed by staffers mentioning euthanasia that he began secretly recording some of their conversations.
In one recording obtained by the AP, the hospital’s director of ethics told Foley that for him to remain in the hospital, it would cost “north of $1,500 a day.” Foley replied that mentioning fees felt like coercion and asked what plan there was for his long-term care…
Foley said he had never previously mentioned euthanasia. The hospital says there is no prohibition on staff raising the issue.
Catherine Frazee, a professor emerita at Toronto’s Ryerson University, said cases like Foley’s were likely just the tip of the iceberg…
Frazee cited the case of Candice Lewis, a 25-year-old woman who has cerebral palsy and spina bifida. Lewis’ mother, Sheila Elson, took her to an emergency room in Newfoundland five years ago. During her hospital stay, a doctor said Lewis was a candidate for euthanasia and that if her mother chose not to pursue it, that would be “selfish,” Elson told the Canadian Broadcasting Corporation.
I don’t claim that this kind of thing is common, but when a financial incentive like this is present, it’s bound to happen, and it’s pretty monstrous when it does.
To me this still reads a bit like an American moral panic. The 27-year-old woman, for example, wasn't granted MAID for being autistic. The ruling was that her autism did not prevent her from making the choice for herself. Her actual conditions, if any, were undisclosed. Similarly, the woman with cancer is facing problems with a badly managed health system, not with MAID. My father is in a very similar situation, and was given treatment immediately and is very happy with the results, those wait times are not normal.
A lot of this seems to come down to whether you view this as a matter of individual freedom. To me what matters is the capacity to make the choice – and depression may be disqualifying then! But I don't understand why I should be forced to live a life of suffering, however I perceive it, just because some other people have terrible arguments about euthanasia being good for the country. You seem to believe that suicide is ALWAYS the wrong choice, except it truly terminal/painful cases, which is a widespread belief but to me, it's a choice you're making for me. When theories came out that abortion causes crime reduction, did you think to ban abortion because that's a perverse incentive?
The concerns I do share are a) using it as an excuse not to fix the health care system at all, which in Canada is facing problems and b) not screening/counseling for capacity to consent.
It's worth quickly flagging that it's not just governments and governmental health care systems that have these incentives. American private insurers would have exactly the same incentives for their most expensive patients to die and stop costing them money. Before the ACA, they would try to kick them off their books and then deny them insurance on the grounds of a pre-existing condition, but since they can't do that any more, trying to get them to die in a way that they can't be sued for malpractice would suit them very nicely thank you very much.